
This article explains the surgical treatments available at American Hospital Dubai for childhood hip dysplasia. If you would like to understand what is hip dysplasia is and non-operative treatment options see our article on Childhood hip dysplasia: non-operative treatment)
If hip dysplasia is diagnosed early it can often be successfully treated without surgery using either a harness or a plaster cast to gently position the hip correctly (see AHD article Childhood hip dysplasia: non-operative treatment). However, if the dysplasia is diagnosed later when the child is of walking age, the chances of successful treatment without surgery decrease. Earlier diagnosis helps to avoid surgery which is why we advise that any baby born with risk factors for hip dysplasia has an ultrasound scan at 4-6 weeks of age.
When hip dysplasia is diagnosed in children of walking age (8 months +), the chances of being able to manually position the hip into the joint reduce significantly. This is usually due to two factors. Firstly, there may be structures within the hip blocking its ability to achieve a normal relationship between the ball and socket. An arthrogram (dye injection study) is usually the best means to determine if the ball (femoral head) can be manually positioned into the socket (acetabulum) so that it is deep and stable. If the arthrogram suggests that the ball can not sit deeply in the socket then it will not be stable and will likely re-dislocate.
The second concern, is that once a hip dislocates it stops developing normally. In the first year of life in a normal hip, the socket deepens and the ball comes to lie in a more stable position as the child grows. The socket deepens making the hip more stable. When the child starts walking around one year of age, standing pushes the hip in deeper which adds to the development.
In the dislocated hip these changes do not occur. The socket remains shallow. Even if there are no structures in the way of the ball getting into the socket, the problem is that often the socket is too shallow to keep the ball in when the child stands. In such a case you may do an arthrogram study and find the ball goes into the socket but it doesn’t want to say there.
Surgery is required to achieve two objectives – (1) Remove any obstructions to place the ball deeply into the socket and (2) Correct the shallowness of the socket and other factors which might cause the hip to re-dislocate. Therefore surgery is only considered if non-operative techniques can not get the ball into the socket or that the ball can be placed into the socket but keeps slipping out.
The exact surgical procedure depends on the age of the child, the severity of the hip dysplasia and the arthrogram (dye study) findings. The surgery usually takes a few hours and the key techniques include:
1. Arthrogram – this is where dye is injected into the hip to determine what obstructions are present to manually placing the ball back into the socket.

Figure: Arthrogram showing needle insertion under x-ray guidance into the hip joint of an anaesthetised child. Injection of contrast dye (black) allows the joint to be visualised and determine if (a) the ball can be placed into the socket and (b) how stable it is.
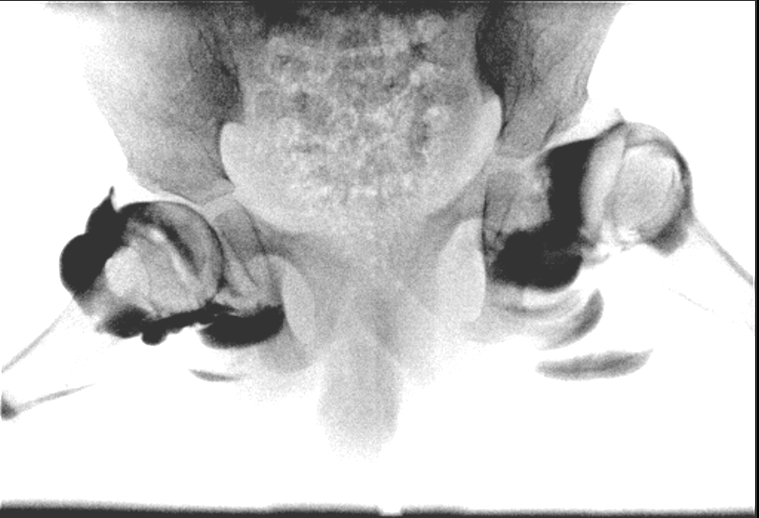
Figure 2 Arthrogram of both hips showing on one side the hip is unstable and can be dislocated easily. As the hip dislocates the socket fills up with the injected contrast dye.
2. Open reduction – this is where the hip is surgically opened to remove obstructions and place the ball deep into the socket. It is done through a “bikini incision” where the scar is in the groin crease and heals with a better cosmetic result.
3. Femoral osteotomy – this is where the thigh bone is shortened and the rotation is corrected to point the ball deep into the socket. It is important to shorten the bone to reduce the pressure on the ball when it is placed into the socket. Shortening the thigh bone makes all the surrounding muscles less tight which means that there is less risk of pressure causing damage to the ball. Shortening is also undertaken to make the leg lengths the same after surgery as the thigh bone is usually longer on the dislocated side. After the thigh bone is shortened and rotated it is fixed with a metal plate. The surgery is done through an incision on the side of the leg.
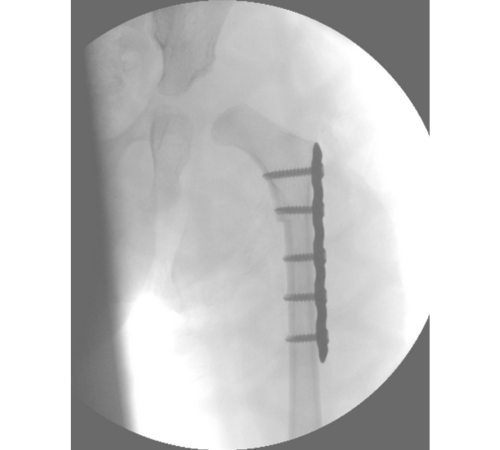
Figure 3. Femoral osteotomy. The femur bone has been divided and shortened by taking out a segment of bone. The femur is then fixed using a metal plate and screws. The femur is fixed with the top part rotated so that the ball points into the joint to make it more stable.
4. Pelvic osteotomy – this is where the pelvic bone is divided and stretched open to make the socket less shallow allowing the ball to sit deeper in the socket and to make it more stable. This is a crucial part of the operation and needs to be done well to have the best outcome. We perform the Dega osteotomy which is the most powerful means of correcting the socket to ensure that the hip develops normally without re-dislocating. The Dega osteotomy does not require any implants or metalwork unlike other osteotomies and is done through the same “bikini incision” as the open reduction.

Figure 4a: Pelvic osteotomy(1). The pelvic bone is divided above the socket using an osteotome (chisel like instrument)

Figure 4b: Pelvic osteotomy(2). The divided pelvic bone is stretched open like a hinge. This brings the roof of the socket down over the head improving the shape of the socket which prevents the hip from re-dislocating.
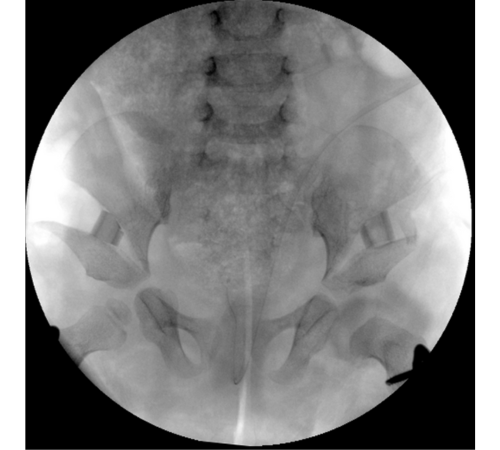
Figure 4c: Pelvic osteotomy(3). The gap from stretching open the division of the pelvic bone is held open by placing a small segment of bone in the gap. This holds the corrected position of the socket roof being lowered without the need for more metalwork such as wires or screws. The segment of bone is actually the piece of bone taken from the femur when it was shortened.
5. Hip spica- at the end of surgery, the child is placed into a plaster cast to keep the hip in the correct position whilst the bone and tissues heal. In many centres the plaster cast may be continued for 3 months or the child may be placed into a brace after coming out of plaster. At American Hospital Dubai we undertake surgery that addresses all the problems and ensures the hip is completely stable once healed at 6 weeks. The benefit to having your child’s surgery at American Hospital Dubai is that they will only be in the plaster cast for 6 weeks following hip dysplasia surgery. At 6 weeks the cast is removed and physiotherapy is prescribed. In the walking age child, you can expect that the child will begin to walk again in a few weeks.

Figure 5: X-ray of the same child 9 months following surgery. The dislocated hip has begun to develop normally and now resembles the opposite side. The osteotomies (breaks) in the pelvic and femur bones have filled in with bone. Both hips have good sockets. The metal plates are usually removed a year after the first operation but are done as a day case procedure with the child going home the same day.
There are potential risks with any surgery. Surgery for hip dislocation is a major undertaking and the doctor will explain general risks of surgery as well as risks specific to the hip joint.
General risks of surgery include infection, need for blood transfusion, nerve or vessel injury and risks of anaesthesia. The risk of infection in childhood hip surgery is less than 1% and we routinely give antibiotics during the perioperative period to minimise this risk. Depending on the scale of surgery some patients may require a blood transfusion after surgery or more rarely during surgery if there are any concerns. The risk of nerve or major blood vessel injury is less than 1%.
Specific risks to the hip during surgery include re-dislocation, avascular necrosis (damage to the ball in the joint) and residual dysplasia (socket remains shallow during development). The accepted risk of re-dislocation is 10% in the literature. However at American Hospital we strive for a 0% re-dislocation rate which we ascribe to undertaking complete deformity correction with femoral and pelvic osteotomies at the time of open reduction.
Avascular necrosis is where damage to the ball of the joint (femoral head) occurs following treatment. It can occur with non-operative or operative treatment but is more common in the latter.A common cause of avascular necrosis is pressure on the ball in the socket following treatment. This damages the blood supply of the hip and over time the ball becomes less spherical and mis-shapen. It can not be reversed and the best strategy is to try to avoid it occurring. At American Hospital Dubai, we undertake careful surgical technique andshortening of the thigh bone at the time of surgery to reduce the tension within the hip jointand minimise the risk of avascular necrosis.
Residual dysplasia is where the socket remains shallow with growth. If severe enough this can cause the hip to re-dislocate. Residual dysplasia often occurs when an open reduction is done without a pelvic osteotomy or using a sub-optimal pelvic osteotomy technique. Many doctors will counsel families that the child may require several surgeries throughout their childhood to address this problem. At the American Hospital Dubai, we believe in correcting the problem properly in the first place. A pelvic osteotomy is always done at the time of open reduction using a powerful corrective technique known as the Dega osteotomy. We aim to treat hips completely in the first instance to limit the number of future surgeries the child will require.
At American Hospital Dubai we have considerable expertise in revision surgery where a hip dysplasia case has been undertaken elsewhere but the desired outcome was not achieved. Usually this is because the hip re-dislocated, the socket remained shallow, there is a leg length difference or a combination of all three. An arthrogram (dye injection test) is a good investigation to define the anatomy and plan corrective surgery to correct the hip anatomy. Revision surgery often involves the same techniques of femoral and pelvic osteotomy to achieve the correct hip anatomy. These techniques are very user dependent. Although a child may have been treated with the same procedure at a different institution, at American hospital Dubai we strive to perform surgery to the best technical standard to ensure the hip anatomy is reproduced and stability is achieved.
Syndromic hip dysplasia is where the hip dysplasia is seen in association with other clinical manifestations of the syndrome. Down’s syndrome, Prader-Willi syndrome, Kabuki syndrome and Arthrogryposis syndromes can all give rise to hip dysplasia which behaves differently to developmental hip dysplasia. Syndromic hip dysplasias are often more difficult to treat and require a modified approach to treatment. The type of surgery has to be calibrated to the underlying cause of the dislocation whether it is joint laxity or muscle contractures. At American Hospital Dubai we have expertise in patient specific treatment plans to address syndromic hip dislocations with good clinical outcomes.
If your child is affected by hip dysplasia, seek a consultation with our Pediatric Orthopedic Surgeons at American Hospital Dubai for best in class care through the below links.

Consultant Pediatric Orthopedic Surgeon
Patient Experience
Chief Arthur Mbanefo, 91 years old, former ambassador to the UN and Representative of Nigeria, thanks the American Hospital Dubai for the excellent medical treatment and personalized care he received.




